The setting is Myrtle Beach, South Carolina, a lovely, ever expanding city that invites tourists and retirees. I am of the latter category. Although a recent transplant, I find myself objecting to the burgeoning housing almost as heartily as a native. But on the other hand, not really, because I have no idea what this coastal town looked like in days gone by, before monster hotels and multi-story condos intruded upon the “Grand Strand” as it is called, wiping out unobtrusive motels and filling up the shoreline with sun blotting structures.
What I do know is that in the two years I have lived here, residential developments have lain waste to acres of forested land; stately pines have been murdered and hauled away to meet their fate in the shredder. Perhaps they will become mulch. But in their absence, the bare, brown ground sits littered with stumps and branches. Birds and other wildlife have evacuated; there is nothing left for them to feed on or nest in. Monsters sit poised upon this land—great excavators and bulldozers await their instructions from greedy developers.
Homeowners in the vicinity weep. I think they do at least, as they see another development going up in their backyards. How quickly they forget that not too long ago, their own pretty neighborhood was a forest. When I say pretty, I don’t mean that at all. Developments less than ten years old are devoid of meaningful foliage. Palmettos planted uniformly grace every front yard. Scrappy bushes pass for hedges. Fake ponds attempt to break up the monotony of beige houses that all look alike.
This is what once proud trees have been sacrificed for.
I live in a condo overlooking a beautiful golf course that has recently been closed. Holes and pipes dot the landscape where manicured greens once welcomed golfers. Soon construction will begin on a new residential development that will feature 220 single family homes. “No Trespassing-Construction Zone” signs have been posted at strategic locations to warn asylum seeking walkers to stay away. The paths along the course are now forbidden territory.
My view of pine trees, luscious Bermuda grass, whimsical sand traps and peaceful ponds will be obliterated. The sounds of excavation and building will disrupt the tranquility I have enjoyed for two years. What was once protected land will be destroyed.
There are almost 100 golf courses in Myrtle Beach. Each course is an oasis amidst the arid landscape of ever expanding residential and commercial development. I am not a golfer, but I enjoy living on a golf course, as many residents do. Several courses were forced to close during the pandemic, and it remains to be seen whether they will reopen or if their owners will be forced to sell to builders. Many homeowners who currently enjoy a golf course view will no doubt have to contend with the decimation of charming vistas.
I am devastated by the take down of defenseless forests. If the lands were destined to be golf courses, the destruction of trees would be a little less painful to me. Just a little. In my own neighborhood in Carolina Forest, several arboreal graveyards along River Oaks Drive will soon house unattractive commercial complexes and nondescript neighborhoods. It is heartbreaking to see once magnificent woodlands wiped out.
As a concerned citizen perhaps it is my duty to make my voice known—to get involved with local groups fighting against further development. For such development will surely affect the environment, strain water and sanitation systems, increase flooding, impact the infrastructure, and put greater demands on emergency services.
I could attend zoning meetings. I could write letters to council members. And yet, it is not fair for me to oppose such development. I would be a hypocrite. After all, I escaped to Myrtle Beach; I sought haven in a place where the weather is warm and beaches beckon year-round. A place where property taxes are low and housing prices are relatively reasonable. So how can I begrudge those who follow in my footsteps? Should they not be allowed to experience all this area has to offer?
In the end, they will come. Perhaps they will not object as I have to the charmless developments springing up throughout the area. It is likely they will, in fact, occupy the beige houses that sit upon land once covered with splendid pine trees. And they will enjoy Myrtle Beach, oblivious as I was to how it looked once upon a time.
This is my verse of comfort tonight after a challenging week. It is my reminder of where I come from, who’s in charge, and who I truly belong to. So much peace in these words.
Be well, friends. ❤️
“For you created my inmost being; you knit me together in my mother’s womb.
I praise you because I am fearfully and wonderfully made; your works are wonderful, I know that full well.
My frame was not hidden from you when I was made in the secret place, when I was woven together in the depths of the earth.
Your eyes saw my unformed body; all the days ordained for me were written in your book before one of them came to be.
How precious to me are your thoughts, God! How vast is the sum of them!
Were I to count them, they would outnumber the grains of sand— when I awake, I am still with you.”
As my pastor mentioned today in his sermon, when everything (including my church) closed down last March, we never thought we’d still be in the midst of this pandemic a year later. Heck, we were thinking we’d be back in church for Easter services. Little did we know…
In Massachusetts, like many other states, the vaccination process is slow going. As many of you probably already know, the guidelines for when certain groups of people get the vaccine is determined individually by each state. What this means is that someone who is a teacher or a restaurant worker, for example, may get their vaccine earlier, or later, in one state as compared to where I live in Massachusetts.
Because of differences in how each state prioritizes their groups and also differences in how quickly a state moves through the phases, I had been watching many of my friends, who have Sjogren’s and other related medical conditions, getting their first, and even second, vaccine doses. So, I was patiently waiting for Massachusetts to get to my phase while I was eagerly keeping track of governor updates because based on what I had seen occuring with the previous groups, I knew it would be a challenging process.
Due to my medical conditions, I am considered high risk for COVID-19. I also fall into the vaccination group of high risk people with two medical conditions as defined by the state and the CDC. I actually have three of the conditions, so there is absolutely no question of what group I fall into. This puts me in the Phase 2B group in Massachusetts, along with the 65+ folks.
It’s hard to wait in anticipation of something that will eventually change so many facets of your life. With some rare exceptions, I have been on lockdown since the first weekend of March 2020. I remember the weekend vividly because it was the last time I had been in a restaurant. My husband and I had gone to one of our favorite local establishments to have lunch with my stepson and his girlfriend. Then, everything got shut down.
Since I have several conditions that make me high risk for either getting COVID-19, or getting sicker than the average person if I do get it, my husband and I have taken the precautions seriously and our entire lives have changed because of it. And the closer I got to the possibility of starting the vaccine process, the harder it got to wait.
I am on disability because of my health, but I do still have a valid nursing license that I keep up-to-date. That license would be all that I would need to get vaccinated in our state’s first phase, which was for medical personnel. Many people encouraged me to do so. If I am being completely transparent, I briefly considered it. I had been isolated for ten months at that point, I was struggling with depression at times, and I was starting to be get more concerned about my mental health than my physical health. I did a lot of praying about it and when I thought about it and listened to what God was saying, it just didn’t feel right. If I was working as a nurse, of course I would have signed up for my vaccine. But, I wasn’t. I could (mostly) stay safely in my house and by doing so, not take a vaccine away from a healthcare worker or person over age 75.
About two days after I made that decision to wait, a friend of mine, who knows my situation, contacted me to tell me that one of the mass vaccination sites in Massachusetts (coincidentally, the one closest to me) was opening up appointments for those with two or more high risk health conditions and 65+. I didn’t understand why since I hadn’t heard anything on the news about it, especially since it was a holiday.
I went to the facility’s direct link my friend gave me and sure enough, you could register for an appointment if you have two or more high risk conditions and there were plenty of appointments to choose from, so I secured an appointment for a Friday afternoon, which is when I wanted to go in case I had a reaction or side effects over the weekend. That was only four days away. However, when I shared the registration link with two people in similar situations, the 65+/high risk option would disappear, reappear, disappear again and they couldn’t register. I started to wonder if it was a mistake or a computer glitch.
A little over 36 hours later, our governor advanced the schedule for the 65+ and high risk groups to be vaccinated, but appointments at the facility I signed up for disappeared almost instantly because so many people were making their appointments directly through the facility’s site. I do know a few people close to me who were able to get appointments at other sites, but the state registration system initially failed and when it finally did go back up, appointments were taken up very quickly.
This would probably be the time to mention that I did not come to this decision to get the vaccine lightly. Like everyone else, I had known about the vaccine for a while and I really struggled in coming to terms with getting it. I am not anti-vaccination by any means. But, I also know enough about science and medicine to know that there was a potential for complications, especially in regards to the autoimmune illnesses I have. What if the vaccine caused more autoimmune issues? Would there be any long-term consequences to getting the vaccine? How long would it work for?
Some of you know that back in 2012, I was stricken with some scary symptoms that doctors could not figure out right away and I ended up being diagnosed with a mild form of Guillain-Barre, a neurological autoimmune disorder which back then, was loosely associated with the flu vaccine. We do not know if that was the cause in my case, but I could have died. And, I was told not to get a flu shot ever again. However in recent years, new research came out that showed the chances of getting Guillain-Barre from a flu shot was LESS than if you got the flu because the flu itself can lead to Guillain-Barre. This was the first season in 10 years I got a flu shot.
These were the kinds of things that concerned me though about the COVID-19 vaccine. That being said, I did a lot of my own research and had conversations with my medical providers, who, despite knowing there have been no trials of the COVID-19 vaccine in autoimmune patients, overwhelmingly suggested I get the vaccine. I also received some valuable information from a person I know very well who has a connection with someone who worked on the Pfizer vaccine and after talking to him and learning more about the technology in developing the vaccine and how long mRNA has been around, I felt more confident that it was the best course of action for me.
Lastly, I thought about the philosophy I have incorporated into my life since my Sjogren’s journey started and that is: don’t let fear of the unknown future prevent you from living today. While I have learned some valuable lessons during this pandemic, I am not safe in this world from COVID-19 without a vaccine.I strongly feel that God wants me back in society as much as my health will allow me to be and he has left this opportunity at my door to do so.
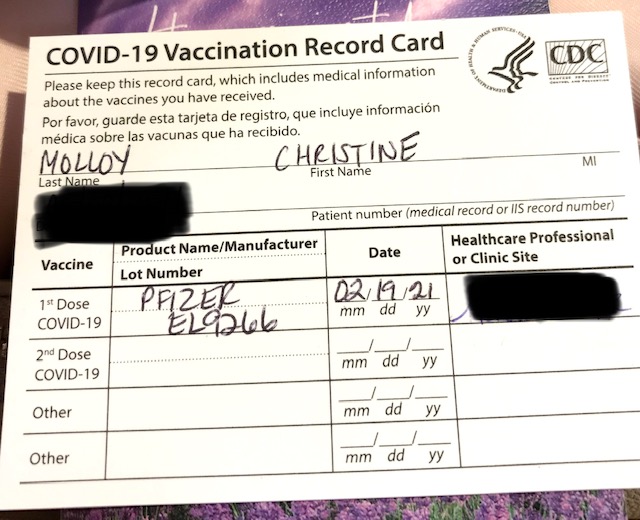
Two days ago, I went and received my first dose of the Pfizer vaccine at a mass vaccination site. I was hoping to get the Pfizer vaccine, but would have taken Moderna as well. My husband drove me for two reasons…because I do have an allergy to CT scan contrast and because we were going during what was supposed to be a winter storm (it fizzled) and if there were going to be wasted doses due to people not showing up, I was hoping he could get vaccinated, which ended up not happening.
The process went much smoother than I anticipated although I have to admit, I was scared. The site wasn’t overcrowded like I thought it would be, there was no wait, and the whole process seemed to be flowing well. I was told that I would have to stay twice as long for observation because of my allergy history, but that actually reassured me that the people doing the vaccinations were on the ball. The injection itself was painless, which was surprising. My blood draws are more painful than the COVID injection. I got a vaccination card, a second appointment for three weeks, and told what to do in the observation area. Hopefully, there will be enough vaccine for my second dose.
Once I sat in the observation area, I almost immediately got a bad headache, which left me pretty quickly, maybe 5-10 minutes later. We picked up some dinner and all was going well until about two-three hours later when my arm started to hurt, a lot. I’ve had a lot of experience with this because as an adult, I’ve had several pneumonia vaccines, tetanus, pertussis, etc., but this was certainly the most pain I’ve ever had from a vaccine. I took some Tylenol and put an ice pack on it, which did help some.
I’m now approaching 48 hours post-vaccination and I have felt worse this weekend than I thought I would, especially since I heard that it’s the second dose that gives you the worst side effects. I’ve experienced what feels like mild cold symptoms, headaches off and on, nausea, one episode of dry heaving yesterday morning, some dizziness, and severe fatigue. Except for the fatigue, none of this has been dramatic and overall has been quite manageable with rest and fluids. Also, you must keep in mind that since I have autoimmune diseases, my body makes a life mission out of attacking my healthy cells on a daily basis, so introducing something like the COVID vaccine is a lot for my body to handle.
So, I wait. I am not considered fully vaccinated until two weeks after my second dose, which like I mentioned, is in three weeks. However even then, I will not be going back to a life of freedom because even if you are fully vaccinated, you can still spread the illness to others and I will not take that chance with my husband, who will be waiting a while to be vaccinated if Massachusetts doesn’t improve the vaccination process. We have had conversations about this and have decided that until he is vaccinated, I will only be adding going to stores (which he has been doing) and seeing my parents (who have been cautious) to my list of limited activities. Church, social gatherings, eating out, events, and other things will have to wait.
I’m more than O.K. with this plan. First, and most importantly, my husband has carried the burden of being married to a high risk person during a pandemic for almost a year now, he has sacrificed a lot, and never once, has he complained about it. Now it is my job to do the same for him.
Second, in addition to Jesus, I’m hanging on to something more valuable than all those other things I listed…
I have hope.
From the moment I clicked that button to complete my vaccination registration to the moment I got that shot, to the moment, I felt my first side effect and thought, “that’s my body building up immunity”, I have felt hope…not for a life that looks like the one I had pre-pandemic, but rather, a life that will be more appreciated and more intentional. A life that will hopefully be more safe.
My prayer is the same for you.
(As an aside, I am off social media for Lent, but my blog posts will be posted. If there is some way I can help you with vaccine appointment registration or navigating the system in Massachusetts, please contact me at cmolloy435@charter.net).
Disclaimer: This post is about my own experience only and information I have learned. intermittent fasting may not be safe or suitable for you, especially if you have any medical conditions. Please consult with your doctor.
Photo credit: Caroline Attwood via Unsplash
My intermittent fasting journey began one year ago today.
I knew nothing about intermittent fasting (also referred to as IF) until a friend of mine, who also has Sjogren’s (an autoimmune disease), posted about it on Facebook. Since starting IF, she had seen changes to her body and improvement in some of her Sjogren’s symptoms. I messaged her and she pointed me in the right direction to get started.
My friend told me about a book, and a corresponding Facebook group, that she found very helpful in learning about IF. That book is Delay, Don’t Deny: Living An Intermittent Fasting Lifestyleby Gin Stephens and it has honestly been one of the most life-changing books I have ever read.
I started doing some research and to be honest, I was skeptical about this whole fasting thing and the claims that were being made about what it could do for your body. Coincidentally, at the same time, I found out about a one hour seminar about IF that was taking place at Massachusetts General Hospital, which is where several of my specialists are and the seminar happened to be right after an appointment I had that day.
I made a point of reading as much of Delay, Don’t Deny as I could before the seminar so I could better understand the mechanisms of how this eating plan worked. Sure enough, the seminar, which was being put on by the weight management department at Mass General, told me a lot of the same information as the book did. There had to be something to this. An important point I would like to make here is that I did discuss IF with two different specialists, who have known me for a while, and they were both on board with it.
I joined the Facebook group that my friend recommended and I was shocked at some of the results I was seeing online; not just weight loss results, but health benefits as well. At this point, my weight was the highest it had been since I met my husband 9 years prior and I was struggling not only with the joint and muscle pain that comes with Sjogren’s, but the associated complications such as irritable bowel syndrome, reflux, and the overall general inflammation that comes with an autoimmune illness. In addition, I have a history of struggling with sugar addiction and polycystic ovarian syndrome.
So what is intermittent fasting?
Many people have the misconception that it is starving yourself or that if you fast, it must only be for religious reasons or because you have an eating disorder. But, intermittent fasting is just that, intermittent. It is a way of eating that is targeted towards changing your metabolism so that you lose fat, retain muscle, and stop damaging your metabolic system with yo-yo dieting.
When we are constantly eating meals and snacks throughout the day, our metabolism is constantly on the go. This food intake also includes all substances we put in our body meaning that it is not just food; it is also all those drinks and mocha latte whatever they are called coffees we drive through to pick up on our way to work or school.
What does this do to the body? It causes our body to constantly produce insulin, often much more than we need. These high insulin levels then result in preventing our bodies from burning our fat stores and continue to keep adding to those fat stores. More insulin production=more fat.
When we fast for a certain period of time (the time depends on many factors), our body does not produce those large amounts of insulin, the glycogen (which is stored glucose) in our liver starts getting used up for fuel and after a period of time, once it is depleted, our body starts using the stored fat for energy instead. Using that stored fat can lead to weight loss and improvement in health for some people.
My explanation here of how IF works is very simplistic. While I understand a lot more of the science behind IF, there are a TON of resources online and in bookstores that provide a better explanation than I can. I highly encourage you to do your own research and talk to your doctor. I found the book I previously mentioned, Delay, Don’t Deny and Gin Stephens’s second book, Fast. Feast. Repeat very helpful, especially since the second book dives more into the science of IF.
Some of the possible benefits of IF are:
Decreased inflammation
Weight loss
Cardiovascular benefits
Straightens out hunger hormones
Helps with metabolic syndrome/PCOS
Improves brain health
And, the list goes on and on. These are not just random benefits that somebody came up with. There is actual scientific research on the positive effects of IF on the body and I encourage you to check out some of the studies done on the benefit of IF on autoimmunity, as well as other medical disorders.
So the big question I get a lot about IF is:
How do you do IF? That is a very loaded question because there is no one way to do IF. There are multiple ways to follow an IF program. I would say the only exception to that statement is that you must do it CLEAN! Fasting clean means that when you are in your fasting stage, you should only take in the following things: medications, black coffee, plain tea (plain means no flavoring at all), and water. That’s it. Anything else can release the production of insulin during your fast and you don’t want that!
Like I mentioned, IF can be done a variety of ways, all of which are explained in the two books I mentioned and on various online resources. Some people fast every single day for various periods of time, some fast every other day, and others only fast for a certain number of days per week. The goal is to find what works best for your body and that does take some trial and error.
When I initially started IF, I only fasted 12 hours a day for the first few days and gradually increased my time. I did get headaches and hunger pains in the beginning. I would say that the first two weeks were the hardest. It took me about two months to sit back and say that this was right for me and that I could (and wanted to) do it for the long haul.
I fast every single day, typically for a minimum of 16 hours, but I average anywhere between 16-22 hours a day. My average is 18 hours a day. I never aim for over 20 hours, but since I have been doing this for a while now, sometimes I’m not hungry and when I check my app, I realize it has been 21 or 22 hours since I’ve eaten. That is a rare occurrence though.
I have done this for a straight year, even on holidays. I choose to fast every day because I have multiple medical issues and I am on a list of medications, some of which can damage my stomach, so I have to eat every day and make sure my doctors remember that I am doing IF. One exception to my 16-22 hours is when I am on antibiotics, steroids, or temporarily have to take a medication that must be taken with food; then I drop my fasts to 12-14 hours a day.
With IF, you can also choose when you eat, which is especially helpful for shift workers. My IF schedule is rarely exactly the same. That being said, I do tend to start fasting around 4-6pm on weekdays and then don’t have anything, except water or green tea, until around 11-12 the following day. This schedule makes me feel my best. Often it means that during the week, I cook dinner, eat early and then sit with my husband while he eats after work. Other times we eat together. I have that flexibility because it’s just the two of us.
On weekends, fasts are typically shorter and/or they start earlier/end later as my husband is home and we’re usually together. That’s the beauty of it though…IF can be altered to fit your lifestyle.
In the year that I have been doing IF, despite a pandemic, some rounds of steroids, a family crisis and many other stressors, I have managed to lose 30 lbs. I think that while most of my fasts were clean, meaning I didn’t take anything in during fasting times, my diet has not been as clean as I would like it to have been in regards to what type of foods I have eaten. But, I’m doing the best I can right now and I am working on improving that area of my life.
I also started taking measurements last February because I know the scale doesn’t always tell the whole story and that can be especially true for people who do intermittent fasting. I took measurements of my hips, waist, bust, and underbust. I didn’t bother with my legs and arms because they don’t hold most of my fat. In total, I lost 14 inches this past year and I can tell the difference by how my clothes fit.
Most importantly, I have several symptoms that I feel IF has improved including reflux, irritable bowel syndrome, and migraines. When I am fasting consistently for 18-19 hours a day, I have ZERO food cravings, and that includes sugar. I have had these cravings for as long as I can remember and there is such a freedom in not having them anymore. When I was doing 12 hour fasts because of a 2 week course of a potent antibiotic, the cravings came back and as soon as I had a few weeks under my belt of the longer fasts, ther cravings went away. I have also experienced that it is easier for me to exercise when I am around the 15-16 hour mark of my daily fast.
I have tried every possible eating plan to not only lose weight, but more importantly, to improve my health and I strongly believe that intermittent fasting is one of the most important tools in achieving my goals. Like I mentioned at the beginning of this article, it may not be suitable for everyone and I don’t believe it is a cure all for autoimmune diseases. I don’t believe anything is. However, it is a very powerful tool on the path to wellness. If you have any questions about IF, please feel free to ask them in the comment section below.
Every week, the leadership in my church take turns writing an essay for the church’s blog, which then gets distributed to us via e-mail. This week’s essay was written by a friend of mine and it struck home for me because it was a topic I had just discussed with a friend and had been thinking a lot about as of late. I hope you enjoy it as much as I did.
We’ve all been in this place… …so I won’t spend too much time explaining it, but let me set the scene. You’re running around all day at work. You rush home to whip together the same dinner you make every week. You drop the kids off for youth group, or practice, or lessons or something. You hit every red light on Memorial Drive, and finally make it to a few stores to buy some Christmas gifts.
This scene repeats itself a handful of times every December. Soon enough, you’re taking the Christmas tree down and you never really had time to enjoy the season. You never paused long enough to truly marvel at the fact that our Savior came to dwell among us.
Hey, that’s me too, and I don’t even have any children. But together, can you and I commit to making this December different? I understand there’s a lot responsibilities that lie before you, but what if we spent even 15 minutes each day thinking about that baby born in a manger?
How would that impact the way we see the Christmas season? How would it impact our relationship with Jesus, and with others?
I’ve often found that the most influential moments in my spiritual life happen when I just sit in uninterrupted silence, and ponder the cross. The benefits of course then show outwardly in my marriage, my work, and everything in between.
I recently heard a line in a song on the radio that I’ve heard a thousand times, “O come let us adore Him.” It stuck out to me in a way it never has before. I had to ask myself, do I actually do that during the Christmas season?
I’m sure the wise men had a lot of things on their plate when they decided to travel a great distance to adore Him, but they didn’t let that stop them from beholding the King of Kings.
“And going into the house, they saw the child with Mary his mother, and they fell down and worshiped him. Then, opening their treasures, they offered him gifts, gold and frankincense and myrrh.”
Matthew 2:11
The Bible
We can learn a lot from those men. By adoring Jesus, worshiping Him, and spending time with Him, I believe that this can and will be the most wonderful time of the year. I believe we will experience the peace and joy that all the songs talk about, because we will be looking to and admiring the Author of peace and joy.
The next time you are like me and tempted to stress and fret about all there is to do before Christmas day, will you take a few moments to adore Jesus? He came, He lived a perfect life, and He died on the cross, so that (among many other things) we could do just that. Adore Him.
Billy Peterson Children’s Ministry Director, LifePoint Church, Chicopee, Massachusetts
(Reprinted with permission from The Pulse: The LifePoint Church Blog, December 3, 2020)
Welcome to For Everything There is A Season where I muse and write about a variety of topics pertaining to this complicated and beautiful journey we call life. Writing, especially when it comes from the heart, has become a passion for me. Thank you for sharing in that passion and taking the time to read.
Although I am a registered nurse, I am not a doctor or advanced practitioner and I am not your provider. The posts on this blog are strictly for informational purposes and do not constitute medical advice. They are based solely on my own experiences, knowledge, and opinions. I am not liable or responsible for any damages resulting from or related to your use of any information from this site.